Senior Care Is Evolving. Are You Prioritizing What Matters?

Your residents are sicker than they were five years ago. Your staff is stretched thinner. Families are analyzing your quality metrics online before they ever schedule a tour. And your reimbursement model is changing whether you're ready or not.
If you're a clinical leader in senior care, none of this is news. According to the 2025 ASHA-August Health clinical leadership survey, 75% of senior living leaders report caring for residents with significantly higher needs than just five years ago. At the same time, 65% cite improving staff quality as their top challenge, while nearly half are already operating within or preparing to join value-based care systems.
The question isn't whether your community will shift to outcomes-based care. It's whether you'll lead that shift in a way that supports your team instead of overwhelming them.
Three Realities Forcing Senior Living to Rethink Outcomes
Reality #1: Residents are coming to you later and sicker. As older adults age at home longer, today's residents often arrive with multiple chronic conditions, complex medication regimens, and higher acuity needs from day one. Many communities are managing skilled-like clinical complexity without the staffing ratios, infrastructure, or reimbursement designed for that level of care.
Reality #2: Families are doing their homework. Families are no longer choosing communities based on availability alone. They're comparing the Centers for Medicare & Medicaid Services (CMS) ratings, reading reviews tied to staffing and safety, and asking pointed questions during tours. One negative review about a preventable incident can influence dozens of potential move-ins. The era of families feeling grateful just to find an available bed is over—they're informed consumers making choices based on outcomes.
Reality #3: Value-based care is already here. Nearly 50% of survey respondents are either operating within or preparing to join value-based care systems, and a growing share are assuming financial risk. This isn't a pilot program anymore. It's becoming the standard way payers expect to work with senior living providers and a broader shift toward accountability for outcomes.
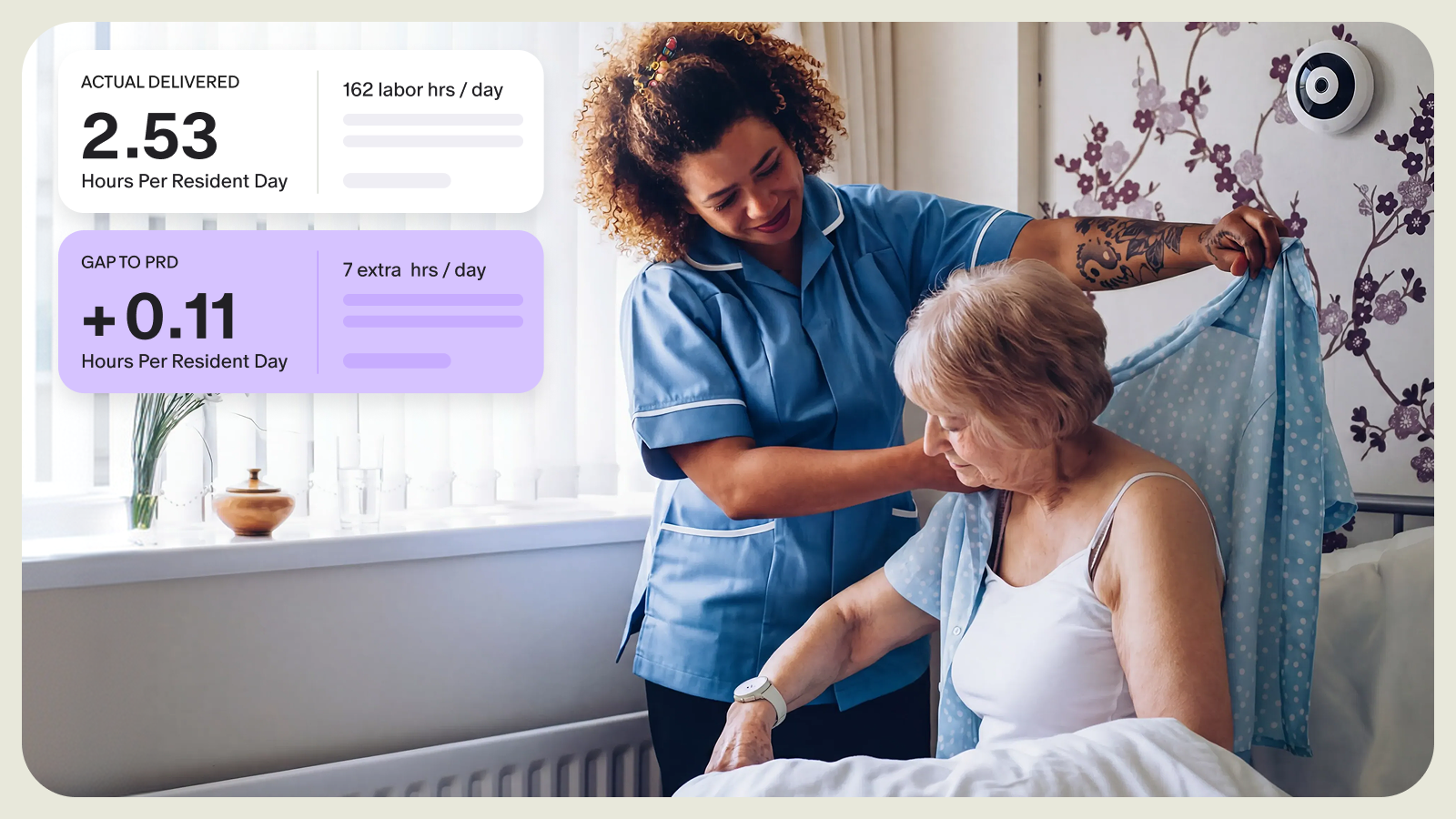
The Assessment Gap
Here's a sobering stat: 68% of clinical leaders believe resident acuity is underreported in their communities due to delayed assessments, intentional underscoring, or undocumented services.
When assessments fall behind, care plans fall out of step. Your team ends up providing more intensive care than what's documented, causing strain, unclear staffing expectations, and lost revenue.
Your Action Framework
The challenges are real, but they're not insurmountable. The shift to outcomes-based care doesn't require a complete overhaul—it requires focus. These four strategies create the infrastructure for proactive, outcomes-based care, while addressing the gaps between what you're delivering and what you're documenting:
1. Fix Your Assessment Process First
What to do: Audit when assessments actually happen versus when they should. If nurses struggle with financial conversations about care rates, separate those roles. Let the business office handle rate discussions after the clinical assessment is complete.
How technology helps: Platforms like Sage can prompt assessments at the right intervals and flag when a resident's condition is changing between assessments— increasing assistance needs, cognitive and behavioral changes—so you're not waiting 90 days to update an outdated care plan.
2. Make Caregivers Your Early Warning System
Your Caregivers see residents more than anyone. They know when someone isn't themselves. However, this intelligence often gets lost in shift change or buried in notes no one reads. By the time the pattern becomes obvious, the resident is in crisis.
What to do: Create simple escalation protocols. Train caregivers to recognize specific warning signs: changes in eating, mobility, mood, confusion, and pain behaviors. Start each shift with a quick huddle: Who seems different today? Who had a rough night? Who needs extra eyes?
How technology helps: Platforms like Sage give caregivers a way to document critical observations at the point of care, routing them to the right clinical team in real time. When observations are aggregated across shifts and caregivers, patterns emerge that would otherwise be missed. The early signals prompt timely assessment and intervention, often before a decline turns into a crisis.
3. Prioritize High-Risk Residents and Build a Data-Driven Culture
The ASHA survey found 88% of leaders recognize that predictive analytics can identify at-risk residents earlier. But only 33% are implementing it. The gap isn't awareness—it's turning data into action.
What to do: Implement weekly 30-minute high-risk rounds. Review who's declined cognitively or functionally, who's on high-risk medications, and who hasn't left their apartment in days... Review community trends: Where are we seeing patterns? Which interventions reduced adverse events? Each session should result in specific interventions. Then track whether these interventions work. Finally, close the loop—show your team the outcomes when their early warnings make a difference.
How technology helps: Platforms like Sage generate your high-risk list automatically and reveal community and portfolio-level patterns. Show your team: "Since we started these rounds, our fall rate dropped 20%." Teams who see their impact stay invested—not because leadership mandates it, but because they've seen it improves resident outcomes.
4. Turn Family Expectations Into Partnership
Families come armed with data from online research. But once their loved one moves in, they often feel in the dark until something goes wrong. Engaged families prevent poor outcomes—they notice changes during visits, provide context about preferences, and reinforce care goals at home.
What to do: When a resident moves in, discuss their actual goals. Not "get stronger" but specific outcomes: walk to the dining room independently, play cards in the activity room, attend their granddaughter's graduation. Update families regularly on progress. When incidents happen, do brief debriefs explaining what happened and what you're changing. Families who feel like partners complain less and collaborate more.
How technology helps: Platforms like Sage empower clinical leadership with early visibility into shifting care needs, facilitating proactive engagement with families. By anchoring discussions in objective, observable trends, leaders can establish clear expectations from the outset. When a concern arises, families receive timely notifications detailing the issue and the care team's response. This transparency shifts the dynamic from a potentially adversarial one to a collaborative partnership.
Start Where You Are
While these trends create real pressure, they also create an opportunity to rebuild care delivery around what actually works. This shift addresses many of the frustrations driving your 50-70% turnover rates. Most caregivers and nurses didn't enter senior care to rush through tasks. They came to build relationships and improve lives. Outcomes-based care, done right, gives them permission to practice the way they always wanted to—with time to prevent crises, tools to spot decline early, and focus on what matters to residents.
You don't need perfect staffing or complete buy-in to start. Pick one thing. Then learn, adjust, and scale.
- Fix your assessment cadence on one unit or care zone
- Implement short caregiver huddles at shift start
- Make early-risk review a standing agenda item in daily huddles
- Start high-risk rounds with your leadership team
The communities that move now will build competitive advantages that compound: better outcomes, stronger staff retention, preferred provider status with payers, and sustained census.
Your residents deserve this. Your staff needs this. And your community's future depends on it.