AI and Data Synthesis in Senior Care: How Sage Is Getting It Right


Why trust, ethics, and responsible design must come before capability, and how Sage is leading the way.
The promise (and the problem) of AI in senior care
Artificial intelligence is transforming industries at a rapid pace. In healthcare, AI is accelerating drug discovery. In finance, it is detecting fraud in milliseconds. In logistics, it is optimizing supply chains at a scale no human team could manage. The excitement is real, and in most contexts, justified.
But senior care is not like most contexts.
When AI enters a senior care community, it is not optimizing a delivery route or flagging a suspicious transaction. It touches on the most intimate details of a person's life: their physical abilities, their medical history, their daily routines, falls and other moments of vulnerability. The stakes are profoundly different, and the margin for error is small.
Yet the need to adopt AI in senior care is very real. Operators are facing new and increasing challenges: chronic staffing shortages, rising acuity among residents, tighter margins, and an ever-growing volume of care data that no team can realistically process by hand. The promise of AI—to synthesize that data, surface early warning signs, and free clinicians to focus on what matters, caring for the residents—is compelling.
The problem is that AI in senior care could easily be leveraged for the wrong reasons, deployed without adequate validation, and trusted before it has earned that trust. The result is a sector where the technology's potential is real, but its risks are just as real. And where the people most affected, residents and their families, have little visibility into how their data is being used.
The core tension: How do you harness the power of AI to improve care outcomes without compromising the privacy, dignity, and safety of the people you serve?
That is the question Sage has been working to answer; deliberately, methodically, and with a genuine commitment to getting it right.
3 reasons why senior care is a high-stakes environment for AI
1. The data is extraordinarily sensitive.
Every day, caregivers in senior living communities generate thousands of data points: care tasks completed, behavioral observations logged, health changes noted. Over weeks and months, this data forms a deeply personal clinical portrait of each resident, capturing not just their medical conditions, but the subtle arc of their physical and cognitive changes.
This is not the kind of data that can be anonymized easily or handled casually. Residents and their families trust communities with information that, in the wrong hands or used in the wrong way, could cause harm. Any AI system operating in this space must treat data protection not as a compliance checkbox, but as a foundational ethical obligation.2
2. The volume of data makes human review alone unsustainable.
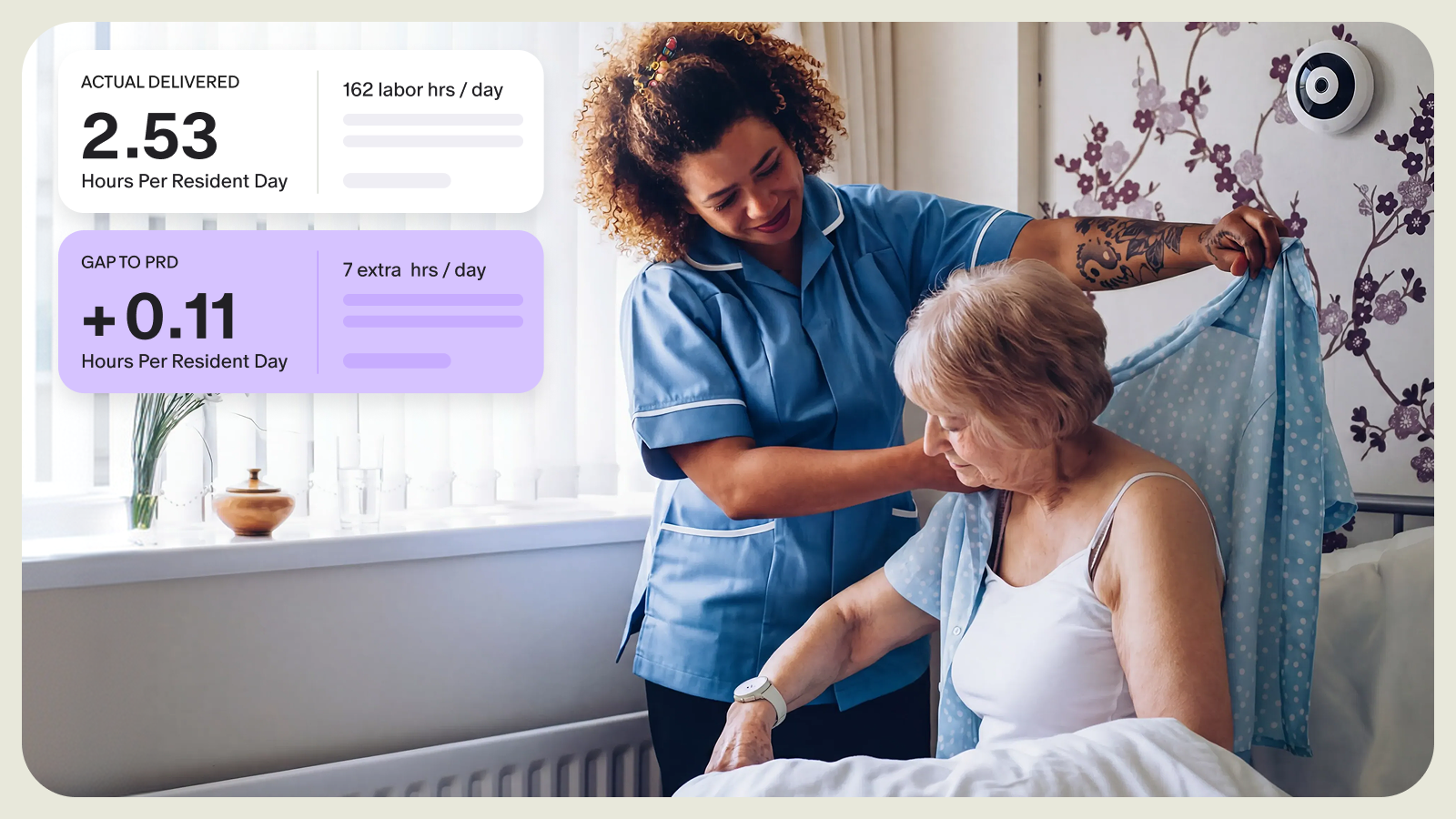
Consider what a single caregiver logs in a month of attentive care: hundreds of individual interactions, observations, and task completions. Now multiply that across a community of 80 or 100 residents. The total volume of care data generated is staggering, and yet a clinician preparing for a resident reassessment must somehow synthesize all of it into a coherent, actionable picture of that resident's evolving needs.
The honest reality is that this is often not feasible without technological support. Important clinical signals, like a gradual increase in fall-risk behaviors, a subtle change in mobility, or an emerging pattern of nighttime restlessness, can easily be missed when buried in thousands of logged events. The cost of missing those signals may be a preventable adverse outcome for a real person.
3. The stakes of getting AI wrong are uniquely high
In many industries, an AI error is a recoverable inconvenience. In senior care, the consequences can be far more serious. An AI system that generates inaccurate clinical summaries could lead a clinician toward the wrong care level for a resident. One that surfaces misleading health trend data could delay a necessary intervention. One that mishandles data could expose residents to privacy violations at a moment when they are least able to advocate for themselves.
This is why the senior living industry needs AI tools built specifically for its context; designed from the ground up with clinical rigor, ethical guardrails, and accountability.
The trust problem: how AI adoption can fall short
Across healthcare and adjacent industries, a consistent pattern has emerged in AI adoption: organizations move quickly to deploy AI capabilities, then discover the hard way that speed and trust are not the same thing.
The failure modes are predictable. AI systems produce confident-sounding outputs that can be subtly or significantly wrong; sometimes these are what’s referred to as "hallucinations," and other times they’re just incorrect conclusions reached because of a lack of appropriate context. Models trained on broad datasets fail to account for the specific populations or clinical contexts they are actually used for. Black-box systems make recommendations that clinicians cannot explain or verify. And data governance practices, often designed for other purposes, turn out to be inadequate for the sensitivity of the information being processed.
The result is a growing skepticism around AI in healthcare. Just deploying impressive technology doesn’t build trust in healthcare. That happens only when you are able to demonstrate, repeatedly and transparently, that the technology works as intended, that its limitations are understood and managed, and that the people using it retain genuine clinical judgment and control.
The fundamental question: Is the AI system making clinicians more effective? Or is it creating new risks under the appearance of efficiency?
Answering that question honestly requires a different approach to AI development: one that starts not with what is technically possible, but with what is clinically valid, ethically sound, and genuinely useful.
How Sage is doing it differently: Our step-by-step approach
Step 1. Listen to clinicians.
We begin by grounding everything in real-world experience. Our team works closely with clinicians to understand where data overload is creating friction, and which insights would meaningfully improve resident outcomes. It’s about starting with need, not technology.
Step 2. Define a focused scope.
AI is powerful, but it is not infallible. We design each feature with clear boundaries, focusing only on the specific insights clinicians need. Just as importantly, we define what the AI should not do, including being directive. Our system synthesizes information and provides helpful facts, data, and trends, which empowers clinicians to do their jobs better. It isn’t intended to replace or automate their judgement. By constraining the scope, we reduce the risk of inaccuracies and ensure outputs remain relevant, interpretable, and clinically appropriate.
Step 3. Build with privacy as a foundation.
From the outset, we design our AI systems so that resident data remains secure and protected. Data generated within Sage is never used to train external models, and all AI-driven insights are governed by the same strict security and confidentiality standards as the rest of our platform.
Step 4. Validate, Validate, Validate
Before any feature reaches our clients, it undergoes rigorous internal testing with our clinical and engineering teams. We then partner with select communities as partners, validating accuracy, usefulness, and real-world performance. If a feature does not meet our standards, it does not move forward.
Step 5. Scale thoughtfully across communities.
What works in one community may not translate directly to another. We test and refine solutions across diverse environments to ensure they deliver consistent value, regardless of community size, structure, or resident population.
Step 6. Roll out with choice and partnership.
New AI features are introduced through an opt-in model. Communities choose whether and when to adopt them, and receive close support throughout implementation. We treat rollout as an extension of validation, continuing to learn, iterate, and improve before expanding availability more broadly. Communities that do not want to implement AI are not pressured to.
Step 7. Continuously improve with transparency.
AI is not static, and neither are we. We continue to refine our features based on real-world use and client feedback. At every stage, we remain transparent about what our AI does, how it works, and where its limitations are, ensuring clinicians remain in control and confident in the tools they use.
Our commitment to data privacy and ethical use
The question we hear most often from operators considering AI is straightforward: “What happens to our residents' data?” It is exactly the right question to ask, and we answer it directly.
- Resident data is never used to train external AI models. The care data generated within the Sage platform belongs to the communities and residents it comes from. It is used to generate insights for them, not to improve third-party systems or create value for anyone else.
- All AI-generated insights are protected with the same security standards as all other resident data within the platform. There is no separate, lower tier of data governance for AI outputs.
- Communities retain full control. Any community can opt out of AI-assisted features at any time. There is no lock-in, no penalty, and no reduction in support.
- We are transparent about what our AI does and how it works. Clinicians understand what data is being analyzed, what insights are being surfaced, and what the system cannot do. We do not ask our clients to trust a black box.
These are not policies we adopted because regulators required them. They are positions we hold because they reflect what responsible AI in senior living actually demands.
The path forward: AI that earns its place
The senior care industry is at an inflection point. The pressures driving the need for AI, including rising acuity, staffing shortages, and an overwhelming volume of care data, are not going away. Neither is the responsibility to deliver care with dignity, precision, and trust.
AI has the potential to meaningfully improve outcomes. It can help clinicians identify early warning signs, make more informed reassessment decisions, and focus their time where it matters most: with residents.
But there are also risks. AI must be introduced thoughtfully. It must be scoped carefully, validated rigorously, and deployed with transparency and control. It must protect the privacy of the people it serves and support—never replace—the clinical judgment of those providing care.
Most importantly, it must earn trust over time.
By taking a deliberate, step-by-step approach, Sage is doing more than just building AI responsibly. We’re building it to set the standard, drive better outcomes, and usher in a new era of senior care.